Like it? Share it!
Common Spinal Dysfunctions and Post Rehabilitation Training
Understanding common injuries and how they occur and the physiology behind them coupled with safe exercise programming will provide an optimal client experience and enhanced function.
Common Spinal Dysfunctions and Post Rehabilitation Training Guidelines
Introduction
Low back pain is a common problem that most people experience at some point in their life. Making it one of the leading causes of functional decline. Whether from an insidious onset or acute trauma, low back pain can dramatically affect one’s life requiring medical intervention, including physical therapy and even possibly surgery. Lumbar degeneration known as arthritis, disc degeneration, disc injury, as well as spinal stenosis are common injuries that I have observed throughout my twenty year career as a physical therapist.
In this article, we will review contributing factors, the pathophysiology of common lumbar injuries, medical management including rehabilitation and safe program design for working with a client who has sustained this specific injury.
Learning objectives:
- Identify the difference between lumbar spondylosis and spinal stenosis.
- Recognize contributing factors that predispose an individual to a low back injury.
- Identify common medical intervention and physical therapy associated with common lumbar injuries.
- Identify, which exercises, are safe vs. unsafe based on biomechanics and science
- Design a Program for a client who has a history of lumbar spndylosis, disc disease or spinal stenosis understanding the science and evidenced based research
Background
Low back pain is one of the most prevalent types of pain that someone can suffer from.
According to the research, in 2012, an estimated 2.06 million episodes of low back pain occurred among a population at risk of over 1.48 billion person-years for an incidence rate of 1.39 per 1,000 person-years in the United States (Waterman et al 2012). The prevalence of spondylosis is on the rise. In a Meta analysis study, a total of 266 million individuals (3.63%) worldwide were found to have degenerative joint disease (DJD) and LBP annually (Ravindra, V, et al 2018). Lumbar spinal stenosis is seen approximately 9.3%, with people most commonly affected in the sixth or seventh decade of life (Schroeder, G, et al 2016).
In the next section, we will discuss three common lumbar injuries. They include lumbar spondylosis(O.A.), disc injuries and spinal stenosis.
Common lumbar injuries
-
Lumbar Osteoarthritis (O.A.)
Pathophysiology: Osteoarthritis also known as lumbar spondylosis, is termed the wear and tear arthritis. Because it is thought that the articular cartilage breaks down because of an imbalance between mechanical stress and the ability of the joint to handle the given loads. Biomechanically, this creates decreased space between the vertebra and possible bone spur development as seen in figure one. Factors that can influence the development of O.A. include; excessive weight, repeated repetitive stressors, and muscle imbalances.
Signs and Symptoms: A deep ache, typically observed at rest, stiffness in the morning that eases or decreases as the day progresses and worsens by end of day. Stiffness and increased tissue density is typically found within the spinal extensors, glute maximus, hip flexors, and hamstring muscles.
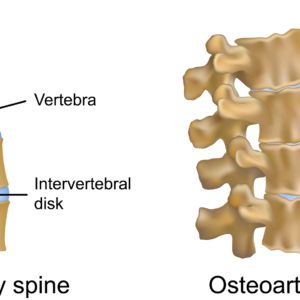
Figure 1. Osteoarthritis (degenerative changes) of spine
Medical Management: NSAIDS (non-steroidal i.e. ibuprofen, Celebrex), are typically given for pain relief. Education is also important on how to reduce of stress to the given joint.
Risk factors: Construction and physical labor position predispose the spine to unnecessary stress, compressing the joint and facilitating spinal degeneration.
Physical Therapy Approach: Physical therapy addresses soft tissue restrictions via the use of myofascial release, soft tissue massage and stretching. Which is to first improve the connective tissue mobility Followed by having the patient stretch tight muscles. The use of stationary bicycle or recumbent bicycle is used to improve mobility and cardiovascular efficiency. The patient is taught how to strengthen weak muscles (transverse abdominis, abdominals, glute medius, glute minimis and core musculature). Pool therapy is effective due to the buoyancy principle, which biomechanically decompresses the spine, while strengthening surrounding musculature.
Recommendations for Training: Aqua or pool therapy is an excellent intervention based upon the buoyancy principle, which unloads the spine. Stretching should be always integrated into working with a client with lumbar osteoarthritis. Emphasis should be placed on targeting the hamstrings, hip flexors, quadriceps, and hip stabilizers (glute medius, minimus and maximus).
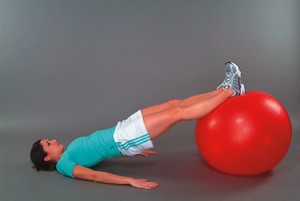
Safe Exercises Include: Lumbopelvic exercises such as planks, bridging with physioball and others are effective in strengthening the core. Horizontal leg press machine and seated leg curl exercises are safe, as they do not place unnecessary loads as a vertical squat machine does.

Unsafe Exercises Include: Vertical squat machine which place unnecessary compressive load to the spine. Shoulder press combined with squatting also places unnecessary compressive load to spine.
-
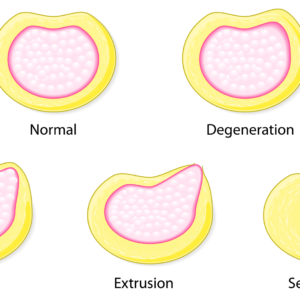
Herniated Disc-Four Types:(Protrusion/Prolapse/Extrusion/Sequestration) Pathophysiology:
- In Protrusion or bulge, there is change in the shape of the annulus that it causes to bulge beyond its normal perimeter.
- In Prolapse disc, the ligamentous fibers give way, allowing the nucleus to bulge into the neural canal. The disc is still contained by the outer layers of the annulus and supporting ligamentous structures.
- Extrusion is where the disc protrudes through the annulus but is contained by the posterior longitudinal ligament (PLL).
- Sequestration is where the nuclear material/free floating piece of the nucleus has partially separated from the remaining nucleus, allowing it to be free in the neural canal and moves into the epidural space.
Etiology/Risk Factors: Overstretching of the annular rings occurs as a result from a combined trunk rotation and unilateral side bending, placing the disc in a vulnerable compromised position. Repetitive compressive forces, micro trauma or one single movement at end range (flexion) with low load may stress the posterior spinal musculature and disc.
Signs and Symptoms: Loss of trunk motion/mobility, decrease in trunk strength, central/radicular pain, possible parasthesias(numbness or tingling) and painful referred pain peripherally and an inability to perform activities of daily living. Pain is usually worse in the sitting position or upon rising.
Medical Treatment: During the acute stage of injury, patient education, rest, and NSAIDS are recommended. Certain positions such as flexion and combined flexion with rotation are avoided to decrease or minimize the intervertebral and disc pressure.
Recommendations for Training: Obtain medical clearance from MD and communicate with client’s physical therapist prior to exercise training. Emphasis is on strengthening of “core,” abdominals, trunk muscles/lower back, and functional strengthening. Avoid combined rotation with side bending exercises, as well as hyper flexion and hyperextension motion.
Effective core exercises including dead bug using physioball, bridging with physioball, or alternate arm with alternate leg lift on physioball just to name a few.

-
Spinal Stenosis
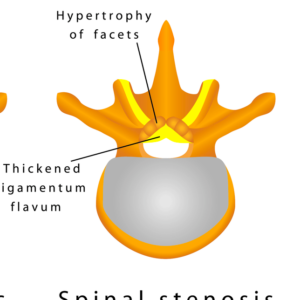
Pathophysiology: Is a narrowing within the vertebral canal coupled with hypertrophy of the spinal lamina and ligamentum flavum or facets as the result of age-related degenerative process as seen in figure 6.
Risk Factors: Poor posture, sitting for long bouts of time (sedentarism), excessive weight, and muscle imbalance between flexors and extensors.
Signs and Symptoms: Results in possible vascular compromise, bilateral pain in lower extremities particularly in back, buttocks, thighs, calves and feet. Pain is increased with spinal extension and walking. Biomechanically, this approximates the spine and causes compression forces to spine. Pain decreases with spinal flexion (bending). Biomechanically, this movement opens the spine, creating space whereby unloads the spine.
Medical Treatment: Conservative therapies initially and if unsuccessful, decompression laminectomies may be required.
Recommendations for Training: Anatomically and biomechanically, flexion-based exercises open the neural foramen. Perform flexion-based exercises such as; knee to chest, prayer stretch and reverse abdominal crunch. End of range extension-based exercises should be avoided as they close the neural foramen (i.e. cobra press-up)
Lower extremity stretching should focus stretching the hamstrings, hip flexors and quadriceps, which are commonly tight in stenotic individuals. Yoga and pilates can also be effective to improve a client’s flexibility and core stability. Progressive resistance training exercises such as lat pull-down, seated mid row, seated reverse flyes, and horizontal leg press machine exercise are all safe to teach a client with lumbar stenosis based on science.
Summary:
Low back pain is one of the leading causes of functional decline that plagues many individuals. Whether from an insidious onset or acute trauma, low back pain can dramatically affect one’s life requiring medical intervention, including physical therapy and even possibly surgery. Understanding common injuries and how they occur and the physiology behind them coupled with safe exercise programming will provide an optimal client experience and enhanced function.
Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, C-IASTM, CPC
Chris is the CEO of Pinnacle Training & Consulting Systems(PTCS). A continuing education company that provides educational material in the forms of evidenced based home study courses, eLearning courses, live seminars, webinars, articles and teaching in-depth, the foundation science, functional assessments and practical application behind Human Movement. Chris is both a dynamic physical therapist with 20 years experience, and a personal trainer with 20 years experience, with advanced training, has created 17 home study courses, is an experienced international fitness presenter, writes for various websites and international publications, consults and teaches seminars on human movement. For more information, please visit www.pinnacle-tcs.com.
References
Hoy, D, et al, 2010, ‘The Epidemiology of low back pain,’ Best Practice and Research Clinical Rheumatology, vol. 24, pp. 769-781.
Ravindra, V, et al 2018, ‘Degenerative Lumbar Spine Disease: Estimating Global Incidence and Worldwide,’ Global Spine Journal, Volume 8, Issue 8, pp. 784-794.
Schroeder, G, et al 2016, ‘Lumbar Spinal Stenosis: How Is It Classified?’ Journal of the American Academy of Orthopedic Surgeons, vol. 24, number 12, pp. 843-852.
Waterman, B., et al 2012, ‘Low back pain in the United States: incidence and risk factors for presentation in the emergency setting,’ The Spine Journal, vol. 12, pp. 63-70.